
Healthcare Insights: Building the Healthcare Workforce of the Future
In February, 2022, I wrote in this column: “Decade after decade, the U.S. recruits millions of people into healthcare professions only to see vacancy rates and shortages skyrocket. Decade after decade, the USA spends up to 20% of its entire GDP on healthcare, yet our population suffers from largely preventable chronic disease, the largest driver of healthcare costs and human suffering. Decade after decade, technology becomes more prevalent, sophisticated, and effective, yet access to this science and technology remains highly disparate based on race, ethnicity, and class.”
“Let’s consider the relationship of the need to transform healthcare from our current state, which still largely is a non-system, which intervenes only after people are sick. Prevention of illness is the centerpiece of healthcare improvement and must be at the center of healthcare transformation. As such, we must learn to think about a transformation of the healthcare workforce as one of the central means to transform care, and to make transformed care available and effective for all patients.” (Scheinman Institute Blog, “Where Did All the Nurses Go?”)
Recently, the Staten Island Performing Provider System (SIPPS) was awarded a $2 million grant from the U.S. Department of Labor. The grant is for a very specific set of healthcare jobs, namely Community Health Worker, Certified Recovery Peer Advocate, Home Health Aide, and Certified Nursing Assistant. These are jobs that are at the heart of a transformed healthcare system, namely one that is designed to prevent chronic health conditions, most of which are related to social determinants of health.
We have known for decades that most health issues that our population suffers from are caused by social determinants of health that lead to chronic illnesses. According to the Centers for Disease Control (CDC), 90% of the $4.1 trillion the nation spends on healthcare is for chronic conditions.
This graphic depicts the definition of Social Determinants of Health: while we often think mistakenly that most of our health issues are related to healthcare, the facts teach us that most of our health issues are related to factors OUTSIDE of the healthcare system:
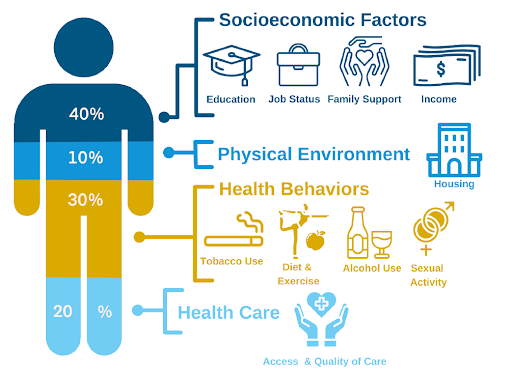
My column today brings together the issues of workforce development and the transformation of healthcare. We cannot transform healthcare without the workforce to execute it, and we will not recruit and retain the workforce we need unless we find the workers to recruit. Furthermore, the new workforce must be provided with the ability and skills to lead the transformed system we must have to prevent illness due to the real drivers of health which are social, economic, and environmental in nature.
Recently Joseph Conte, executive director of SIPPS, announced that:
“The SIPPS is honored on being awarded the Apprenticeship Building America Grant. The U.S. Department of Labor (DOL), Employment and Training Administration (ETA) has recognized only 30 organizations across the nation to receive this funding. It is an acknowledgement of the PPS’s commitment to supporting those affected by disparities and healthcare employers who are struggling to fill positions. The apprenticeship model is an excellent approach to providing economic opportunity to those in need and supporting healthcare employers as they search for new team members to fill in gaps left by COVID. This award focuses on positions to support substance use disorder providers, nursing homes and home health agencies who have been especially hard hit and to expand our apprenticeship program throughout New York State and beyond.”
He added that the “Staten Island Performing Provider System has received the Apprenticeship Building America (ABA) federal grant award from the United States Department of Labor for $2 million over 4 years for four apprenticeship titles: Community Health Worker (CHW), Certified Recovery Peer Advocate (CRPA), Home Health Aide (HHA), and Certified Nursing Assistant (CNA). This grant award will further support the efforts from SIPPS to fill workforce gaps brought on by the COVID-19 pandemic and will streamline the process from training to employment. The goal is to increase the number of registered apprentices by 500 in apprenticeable occupations throughout the region.”
In 2018, ILR Faculty Harry Katz, Phoebe Strom, Ariel Avgar, Adam Litwin, and I conducted a research project with the SIPPS. The project sought to understand the impact of clinical, departmental, and functional integration of healthcare delivery under the Medicaid Delivery System Reform Incentive Program (DSRIP) of which SIPPS was a participant. DSRIP was the primary initiative of NY State Medicaid Reform which sought to reduce hospital admissions by 25 %, from 2014-2020. The state and federal government invested eight billion dollars in physical, technical, and human infrastructure, and gained a return on the investment of $17 billion.
The SIPPS was one of 25 Performing Provider Systems (PPS) which organized care for all of the state’s Medicaid recipients, the second highest number in the nation (after California). This was a grand and huge experiment in healthcare transformation based on the notion that integration of healthcare services across a region would improve health and reduce costs. The experiment was a great success as shown by the ROI cited above.
The Cornell-ILR survey included 671 respondents across 24 facilities. The survey measured employee knowledge of DSRIP, attitudes about the integration of care (occupational, clinical, inter-facility), staffing, training, technology, and well-being.
By and large the results indicated positive outcomes of the various forms of integration from the employees’ perspectives, including increased satisfaction, improved clinical practice, and less stress.
In as much as Cornell-ILR and its Scheinman faculty and staff have had a strong working relationship with SIPPS, it is fitting and exciting to report on the recent continued success of the SIPPS, especially on the topic of workforce development that is integrated into the transformative healthcare delivery that the SIPPS continues to provide to the poor and vulnerable population of Staten Island even after the DSRIP program ended in 2020. I had the opportunity to interview Joseph Conte, to learn about the USDOL Grant award and its strategic importance.
Conte has had a long career as a healthcare executive. His lifelong professional focus has been the improvement of quality for patients as well as the development of technology to enhance opportunity for quality improvement, especially among the most vulnerable members of our community.
I asked Joe why the SIPPS is referred to as a “Learning Management System” (see SIPPS website). He indicated that “at the core of our effort is to focus on population health. And we know what detracts from the health of the population are the social determinants of health, not medical services. In order to improve health, we must understand the surroundings in which people live.”
The concept of a Learning Management System is at the heart of the SIPPS approach to workforce planning and development. With this approach, it’s critical to understand the social determinants of health. To intervene with the population in their surroundings requires having staff who work with people in the community BEFORE they become sick and in need of expensive medical care.
To illustrate the significance of the impact of social determinants of health, look at the following graph. It represents data from 40,000 respondents from Staten Island who were contacted by health navigators recruited and trained for this purpose under the DSRIP Program.
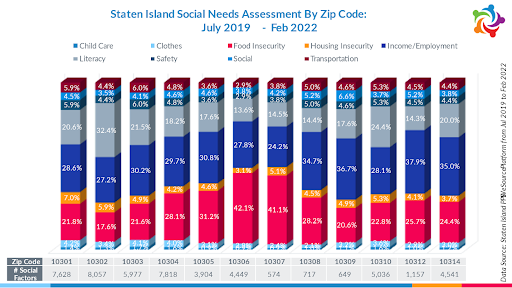
The approach that SIPPS undertook to understand the social determinants of health through its survey provided an opportunity for respondents to lay bare the underlying causes of the social determinants of health.
Joe and his team made a breakthrough from the stereotypical views that many people have about the social determinants of health and recognized that at the heart of social and physical vulnerability is the lack of a decent job! The chart shows that the two most common responses as to the root causes of social needs are: Income/Employment and Food Insecurity.
When we recall that the purpose of DSRIP was to reduce hospital admissions in the Medicaid population by 25%, the primary strategy is to take preventative measures. The SIPPS team focused on key preventive measures such as addiction intervention and rehabilitation, keeping nursing home residents healthier and encouraging palliative care, and improving the health of the homebound and isolated.
However, to accomplish these important functions, a whole new workforce had to be recruited and educated to carry out these preventive functions. In this area, SIPPS created truly innovative approaches to recruit and train the workforce necessary to do this work. The key jobs included:
- Home Health Aides
- Certified Nursing Assistants
- Certified Peer Recovery Advocates (CPRA)
- Community Health Workers (CHW)
These four categories of jobs have much in common: low pay, high turnover, and in the case of CPRAs and CHWs very few even existed.
Among the most important innovations by SIPPS was to make the connection between what was learned in the Social Needs survey: reach out to the thousands of people who complained of employment and income insecurity, and recruit them to become the workforce that was needed to carry out the very type of work needed to address to prevent illness.
SIPPS developed a database of 90,000 phone numbers of vulnerable people: 40,000 who were respondents to the Social Needs survey, and another 50,000 from screening of people in the community done by partner Community Based Organizations (CBOs) who were paid and coordinated by SIPPS from the original DSRIP funding. The SIPPS-developed database has been used by other employers looking to fill jobs and has become a recognized resource for recruitment for the innumerable vacancies in health care jobs created by the pandemic.
Among the successes of the SIPPS Workforce Development Program include:
- Over 70,000 hours of training to upskill workers from 75 employers
- First ever program combining cultural competency, health literacy and LGBTQ sensitivity training to over 20,000 employees
- Created first certified recovery peer advocate (CRPA) program on SI that recently received DOL approval as apprenticeship program
- Developed the first Federally Approved Certified Nursing Assistant Program in New York State, 100% pass rate state exam
- Improved skills of new hires, improved organizational acclimation, reduce turnover and improve employee morale
- Home Health Aide field became a career ladder to CNA
- First round success, led to partner request for second and third cohort in Winter 2019, including building an LPN Apprentice career ladder
- 10 CNA Apprentices started as of January 2020 – Eger, Carmel, Clove Lakes
- SI PPS selected to advance to funding round for NYS Workforce Grants
(from SIPPS website)
One of the central features of the SIPPS Workforce Development program is that it coordinates education and training for jobs across employers and across the borough of Staten Island designed for specific areas of intervention and prevention of illnesses that would otherwise require expensive and unsatisfactory hospitalization. In so doing, the newly recruited workforce is deployed across facility boundaries to achieve true population health outcomes. Two examples are worth illustrating:
At the beginning of the DSRIP Program in 2014, Staten Island was the epicenter of the opioid overdose crisis in the five boroughs of New York City. SIPPS made addiction intervention a priority under the DSRIP program. SIPPS recruited and trained 75 Certified Peer Recovery Advocates (CPRA) who were assigned to hospital emergency rooms, police precincts, and community-based organizations. The job of the CPRA is to get the patient into treatment so as to keep them from needing to return to emergency rooms or wind up in police lock up. The program resulted in a 27% reduction of emergency room admissions in its first three years of operation (2014-2017), and the work continues its success to this day. (For the full report, see the SIPPS website at the tab on “Behavioral Health and Opioid Response”).
Sepsis is a deadly hospital/health facility acquired infection. Under the auspices of the SIPPS in coordination with ten skilled nursing facilities, remarkable prevention of sepsis was achieved. The staff across the ten facilities were trained in the initiative and then undertook uniform improvement projects across the facilities. The results:
“Context: Sepsis hospitalizations with subsequent skilled nursing facility (SNF) admissions have had an annual cost of $41 billion in the United States. There has been a limited amount of literature on early interventions for sepsis in long-term care.
Objective: To assess the impact of a pilot sepsis quality improvement program (SQIP) aimed at early identification and intervention in 10 partnering SNFs in New York City.
Methods: Obtained baseline data of sepsis hospitalizations in 2017 among 10 SNFs. A SQIP was implemented utilizing the systemic inflammatory response syndrome criteria with a modified threshold temperature of 37.2°C (99.0°F). Sepsis hospitalizations were reported and validated for the intervention period in 2018 and compared to the baseline. A cost savings analysis was completed by utilizing local hospital billing records.
Findings: Overall, there was a reduction of 54 sepsis hospitalizations when comparing the intervention period (183 sepsis hospitalizations) to the baseline (237 sepsis hospitalizations), a 22.8% decrease (p < 0.001). The initial SQIP costs were $45,000 USD. The SQIP had an estimated cost savings between $1,039,662–$3,188,430 USD.”
(“Reducing Sepsis Hospitalizations through a Standardized Quality Improvement Program in Skilled Nursing Facilities”, Mary Han, Salvatore Volpe, Alexandra Zamorin, Patricia Tooker, Joseph Conte, Journal of Long Term Care, (2021, pp. 329-338)
SIPPS has practiced what is necessary to create the workforce needed for a transformed health system that is coordinated and integrated to prevent illness and injury based on social determinants of health. It is a model for other health systems to learn from.
Health and healthcare must improve, and in doing so it must become more affordable and accessible. The direction for these aspirations is clear: Our healthcare must be based on prevention through support and intervention of people BEFORE they need medical care. As we rebuild the workforce decimated by vacancies and burnout, we must build a workforce that possesses the skill and capacity for the essentials of preventative care.
These must be high paid and secure jobs not just because we know that job and income insecurity is the largest contributor to ill health that we have, but also because these jobs will create enormous value by reducing the need for expensive medical care as we keep our population healthier.
This workforce development plan, which connects good jobs to prevention strategy, is the WIN-WIN of healthcare transformation. Because it is founded on response and intervention to the social determinants of health.
About the author:
John August is the Scheinman Institute’s Director of Healthcare and Partner Programs. His expertise in healthcare and labor relations spans 40 years. John previously served as the Executive Director of the Coalition of Kaiser Permanente Unions from April 2006 until July 2013. With revenues of 88 billion dollars and over 300,000 employees, Kaiser is one of the largest healthcare plans in the US. While serving as Executive Director of the Coalition, John was the co-chair of the Labor-Management Partnership at Kaiser Permanente, the largest, most complex, and most successful labor-management partnership in U.S. history. He also led the Coalition as chief negotiator in three successful rounds of National Bargaining in 2008, 2010, and 2012 on behalf of 100,000 members of the Coalition.